


Abstract
Background: The COVID-19 pandemic and nonpharmaceutical interventions that reduced the spread of infection had impacts on social interaction, schooling and employment. Concerns have been raised about the impact of these disruptions on the mental health of high-risk groups, including birthing parents of young children.
Methods: This population-based, repeated cross-sectional study used health administrative databases in Ontario, Canada, to link children to birth parents and to measure subsequent mental health visits of birthing parents of younger (age 0–5 yr) and school-aged (6–12 yr) children. We used a repeated cross-sectional study design to estimate expected rates for visits to physicians for mental health diagnoses, based on prepandemic trends (March 2016–February 2020), and to compare those to observed visit rates during the March 2020–November 2021 period of the pandemic.
Results: We identified 2 cohorts: 986 870 birthing parents of younger children and 1 012 997 birthing parents of school-aged children. In both cohorts, observed visit rates were higher than expected in the June 2020–August 2020 quarter (incidence rate ratio [IRR] 1.13, 95% confidence interval [CI] 1.10–1.16; and IRR 1.10, 95% CI 1.07–1.13, respectively), peaked in December 2020–February 2021 (IRR 1.24, 95% CI 1.20–1.27; and IRR 1.20, 95% CI 1.16–1.23) and remained higher than expected in September 2021–November 2021 (IRR 1.12, 95% CI 1.08–1.16; and IRR 1.09, 95% CI 1.06–1.13). The increases were driven mostly by visits for mood and anxiety disorders, and trends in increases were similar across physician type, birthing-parent age and deprivation quintile.
Interpretation: The COVID-19 pandemic was associated with increased mental health visits for parents of young children. This raises concerns about mental health impacts and highlights the need to address these concerns.
The sudden onset of the COVID-19 pandemic in March 2020 generated global concern and resulted in the widespread imposition of a series of nonpharmaceutical interventions (NPIs) to reduce person-to-person transmission of the SARS-CoV-2 virus. These NPIs included stay-at-home orders, restrictions on external and family gatherings, school and day care closures, cancellation of public events, local and international travel restrictions, and closure or restrictions of many economic sectors.1 In Ontario, stringent NPIs were rapidly deployed in March 2020, were eased later that calendar year but ramped back up in early 2021, to be eased again later that year.2 The uncertainty and concern about the pandemic and the fundamental changes to social and family interaction, education and employment stemming from long-term imposition of NPIs raised concerns about the mental health impacts of the pandemic and efforts to control it,3–5 particularly impacts on depression and anxiety3,5 and in vulnerable and at-risk populations.6,7
A 2022 World Health Organization report8 and a 2023 meta-analysis9 showed that the COVID-19 pandemic and efforts to control it had a larger impact on the mental health of women or female participants than men or male participants. A specific area of concern regarding the mental health of women and maternal caregivers during the COVID-19 pandemic is related to their role in child care and parenting. 10,11 Parenting is both rewarding and stressful, and owing to social constructs regarding parenting, women often play different roles than men and report more stress and fatigue related to parenting than men.12 Mothers of young children (age 0–5 yr) or school-aged children (6–12 yr) are at risk for both parenting-related anxiety and depression.12,13
Cohort studies from several countries based on surveys early in the COVID-19 pandemic found increased levels of mental health symptoms and concerns in mothers with young and school-aged children, and suggested that risks may be higher in deprived or racialized populations.14–19 A Canadian study found that the pandemic was associated with job loss in mothers of young children.20 A population-based study in Ontario showed increased use of mental health services by patients in the immediate postpartum period early in the pandemic. 21 Another Ontario population-based study found that virtual care increased rapidly at the outset of the pandemic, but that the total use of mental health services (i.e., the total of in-person and virtual visits) decreased at the outset of the pandemic and remained lower 9 months into the pandemic.22
Our population-based, repeated cross-sectional study uses linked health administrative databases on mental health services (both virtual and in person) in Ontario for 2 large cohorts: birthing parents of younger children (age 0–5 yr) and of school-aged children (age 6–12 yr) before and after the pandemic, to examine the extent to which the sudden onset of the pandemic and the attendant anxiety, along with the rapid and ongoing application of NPIs over the next 2 years, were associated with abrupt and prolonged changes in mental health visit rates.
Methods
Setting
The World Health Organization declared a global pandemic on Mar. 11, 2020, and Ontario declared a state of emergency on Mar. 17, 2020,23,24 and instituted a series of NPIs from that date onward. We used those dates to define 16 quarters from March 2016–May 2016 to December 2019–February 2020 as the prepandemic period, and the following 7 quarters — from March 2020–May 2020 to September 2021–November 2021 — as the pandemic period.
Statistics Canada developed an index that assessed the extent of restrictions imposed by NPIs across 15 dimensions, including school closures, day care closures, restrictions to internal and external gatherings, workplace closings and stay-at-home requirements, measured daily at the provincial level from March 2020 through 2021.2 The summary restriction index for Ontario during the pandemic period is provided in Appendix 1, Supplemental Figure 1 (available at www.cmajopen.ca/content/11/6/E1093/suppl/DC1), which shows how the restriction index waxed and waned in Ontario over the postpandemic period. The Statistics Canada report2 provides detailed timelines for each of the 15 NPIs included in the index.
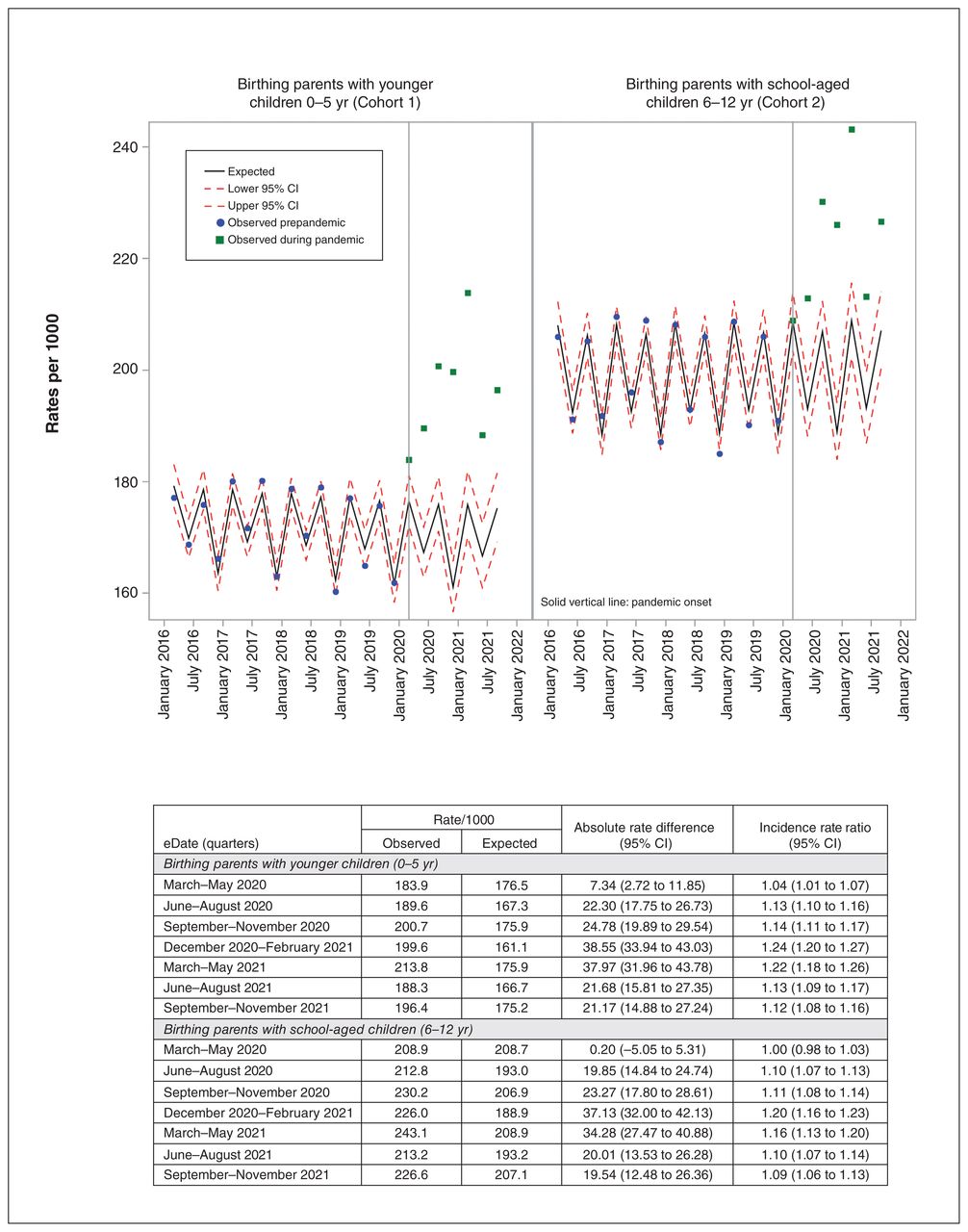
Total expected and observed outpatient mental health visits over time. Note: CI = confidence interval, IRR = incidence rate ratio.
A systematic review and other literature on mental health symptoms in birthing parents during the pandemic suggested that mental health challenges were related to whether the children were preschool aged or school aged.13,16,25 Given this, we defined 2 study cohorts: birthing parents with younger (preschool aged) children, aged 0–5 years; and birthing parents with school-aged children (aged 6–12 yr).
The Ontario Health Insurance Program (OHIP) provides coverage for many health care and medically necessary services, including mental health services provided by physicians to Ontario residents. Physicians were able to bill OHIP for either in-person or virtual visits in both the prepandemic and pandemic periods.
Study design and data sources
We used linked health administrative databases to conduct a population-based, repeated cross-sectional study for all birthing parents with children (aged 0–12 yr), living in Ontario, Canada, and eligible for provincial health insurance between March 2016 and November 2021. Databases used in the study included the provincial health insurance database (OHIP), which contains billing records for all mental health services provided by family physicians and psychiatrists. The cohorts of birthing parents with children were identified using the Mother–Baby Database (MOMBABY). MOMBABY uses the Discharge Abstract Database to link each child born in a hospital to the person who gave birth to that child. The MOMBABY database includes more than 98% of births in the province26,27 and has been used in previous studies of outcomes in birth parents.21
The 2016 Ontario Marginalization Index (ON-Marg) provides a composite measure of income, education, single-parent families and housing quality, expressed as quintiles (1: least deprived; 5: most deprived) at the dissemination-area level.28,29 Each dissemination area is a small, relatively stable geographical unit consisting of 1 or more adjacent dissemination blocks, with a population size between 400 and 700 people.30 Each parent was linked to a deprivation quintile based on their dissemination area of residence. These data sets were linked using unique encoded identifiers and analyzed at ICES.
We used open cohorts and assessed at-risk time to allow individuals to contribute time at risk for outcomes. We excluded people with missing information on encrypted ID, birth date, sex, OHIP eligibility, nonresident, admission or discharge from long-term care facilities during the study, or who had died before the index date. For each birthing parent, we obtained age at the individual level and material deprivation at the area level. Henceforth, birthing parents will be referred to as “parents.”
Study outcomes
The primary outcomes were outpatient visits for mental illness to a primary care provider (general practitioner or family physician [GP/FP]) or to a psychiatrist, derived from OHIP billing claims.31 Physicians can bill for both virtual and in-person visits and we included both in the analysis. Virtual visits accounted for about 10% of mental health visits before the pandemic, and this increased to about 70% after the onset of the pandemic (Appendix 1, Supplemental Table 1). We divided mental health visits into 4 categories, based on diagnostic codes: mood and anxiety disorders, alcohol and substance abuse disorders, other nonpsychotic mental health disorders, and mental health–related social problems (Appendix 1, Supplemental Table 2: diagnostic codes).
Sociodemographic characteristics of study population
Statistical analysis
Using negative binomial regression with time and season as predictors, we modelled utilization trends in the prepandemic period (March 2016–February 2020) and visit rates per 1000. We used the number of eligible parents in each quarter as the denominator. We modelled residuals as an autoregressive AR1 process to account for serial correlation among observations and to account for seasonality. We then used the fitted model to predict the expected rate of visits for each quarter from March 2020 to the end of November 2021. We calculated actual observed rates of use during the pandemic compared with expected rates of use based on the model. We calculated incidence rate ratios (IRRs) and their 95% confidence intervals (CIs). We stratified results from the primary analysis by physician type, diagnosis type, age of parent and material deprivation of parent area of residence. Data preparations, analyses and visualizations were performed using SAS 9.4 and Microsoft Excel.
Ethics approval
The study was approved by the Research Ethics Board at the University of Toronto (RIS Human Protocol No. 41386). This study followed the Reporting of Studies Conducted Using Observational Routinely Collected Health Data (RECORD) guidelines.32
Results
A total of 1 423 931 birthing parents with young children were included in the study, with 986 870 having younger children aged 0–5 years, 1 012 997 school-aged children 6–12 years, and 575 936 having both. As shown in Table 1, most parents of younger children (60.0%) were between age 27 and 36 years and few were older than 48 years. Many parents with school-aged children were in the 37–47-year age group (53.8%) with very few younger than 18 years. The areas of residence for both cohorts were distributed across the deprivation quintiles.
Changes in overall outpatient mental health service utilization
For parents of younger children (aged 0–5 yr), observed rates for mental health visits exceeded expected rates from the onset of the pandemic (March 2020) (Figure 1). The first quarter was slightly higher relative to expected rates by IRR of 1.04 (95% CI 1.01–1.07; 183.9 v. 176.5/1000). Subsequent quarters were also significantly higher and peaked in the December 2020–February 2021 period at IRR 1.24 (95% CI 1.20–1.27; 199.6 v. 161.1/1000) and remained higher at the end of follow-up (September 2021–November 2021) at IRR 1.12 (95% CI 1.08–1.16; 196.4 v. 175.2/1000).
For parents of school-aged children (aged 6–12 yr), observed rates were no different from those expected in the first quarter of the pandemic. However, observed rates for overall mental health service use were higher from the second quarter of the pandemic onward. The highest difference in observed versus expected rates for service utilization was in the quarter of December 2020–February 2021, with an IRR of 1.20 (95% CI 1.16–1.23; 226.0 v. 188.9/1000), and remained significantly higher at the end of follow-up (September 2021–November 2021 IRR 1.09 [95% CI 1.06–1.13]).
Changes in mental health service utilization by diagnosis
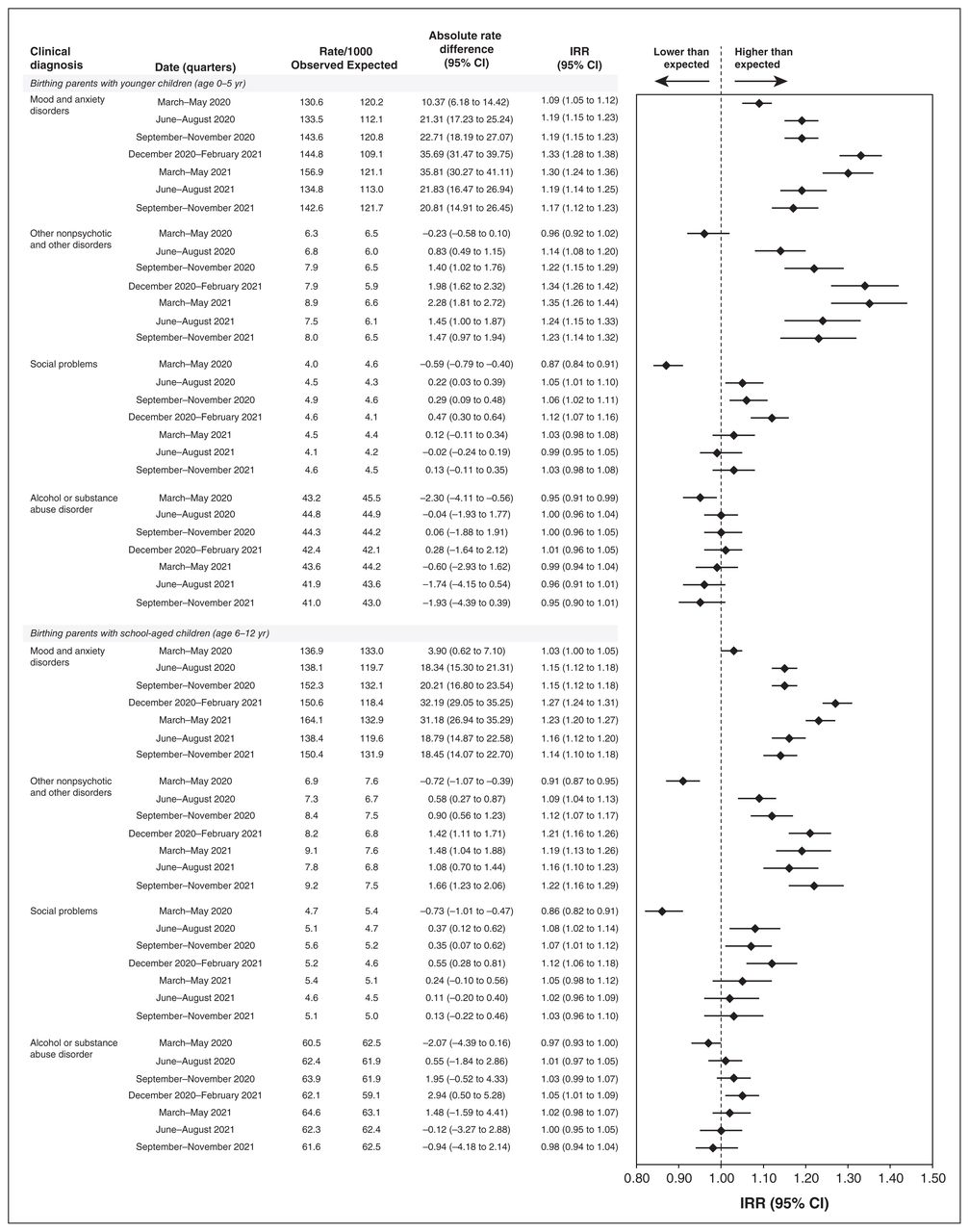
Visits for mood and anxiety accounted for about two-thirds of total visits, and visits for alcohol and substance abuse about one-quarter (Figure 2). In parents of younger children, there was significantly higher than expected service use for mood and anxiety disorders, starting from the first quarter of the pandemic (March 2020–May 2020) and peaking in the December 2020–February 2021 quarter (IRR 1.33, 95% CI 1.28–1.38). This higher than expected rate in service use for mood and anxiety disorders continued for the duration of study follow-up. For other nonpsychotic mental disorders, visit rates were lower than expected in the first quarter of the pandemic but higher than expected thereafter, peaking in the March 2020–May 2020 quarter (IRR 1.35, 95% CI 1.26–1.44). There were higher than expected rates of use for social problems in 3 quarters, but no significant increases for alcohol and substance use disorders.
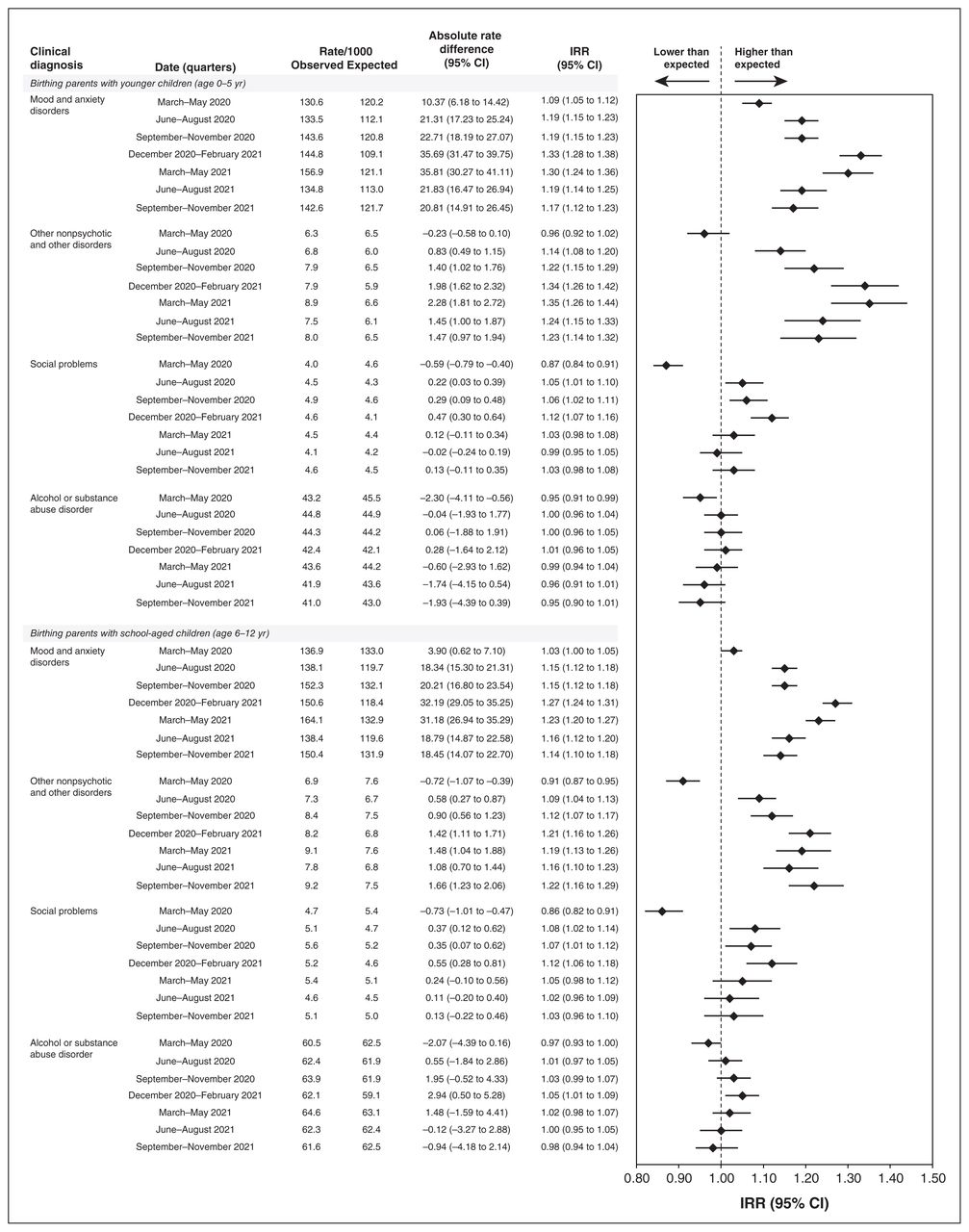
Expected and observed mental health visits by diagnosis over time. Note: CI = confidence interval, IRR = incidence rate ratio.
In parents of school-aged children, rates were not significantly higher than expected for mood and anxiety until the second quarter (June 2020–August 2020), peaked in December 2020–February 2021 (IRR 1.27, 95% CI 1.24–1.31) and remained higher than expected to the end of follow-up. Service use for other nonpsychotic mental disorders were above expected rates for all quarters except for the first quarter of the pandemic, with the largest difference observed in December 2020–February 2021 quarter (IRR 1.21, 95% CI 1.16–1.26). The difference in observed versus expected utilization for social problems was higher in the same 3 quarters than that for parents of younger children, and again, similarly to that cohort, there were no significant increases for alcohol and substance use disorders.
Changes in mental health service utilization by physician type
Overall, about 80% of total visits were to GP/FPs (Figure 3). In parents with younger children, there were higher than expected rates of visits to both GP/FPs and psychiatrists throughout the pandemic, with the IRR higher for psychiatrists in each quarter. In parents with school-aged children, rates did not increase significantly until after the first quarter, and the differences in IRR between GP/FPs and psychiatrists were less pronounced.

Expected and observed mental health visits by physician type over time. Note: CI = confidence interval, GP = general practitioner, IRR = incidence rate ratio.
Changes in mental health service utilization by age of parent
Overall, there were similar patterns of increased use beyond expected across all age groups in both cohorts (Appendix 1, Supplemental Figure 2). The largest increase in parents of younger children was for parents aged 27–36 years in December 2020–February 2021 (IRR 1.29, 95% CI 1.26–1.32), and for parents of school-aged children for those aged 27–36 years in December 2020–February 2021 (IRR 1.23, 95% CI 1.20–1.26).
Changes in mental health service utilization by deprivation quintile
There was an increasing gradient in utilization rates across deprivation quintiles, with those living in the most deprived areas having the highest rates and those living in the least deprived having the lowest rates (Appendix 1, Supplemental Figure 3). After the pandemic period, there were significant increases in use across all quintiles in both cohorts. The highest absolute increase was in those living in the most deprived neighbourhoods and the highest relative increases in those living in the least deprived neighbourhoods.
Interpretation
Shortly after the onset of the COVID-19 pandemic, there was an increase in use of mental health services by parents of younger children in Ontario compared with previous rates of use, and this increase persisted through the next 21 months. This rapid and prolonged increase was observed in parents of both younger children and school-aged children. The relative increase was similar for visits to both primary care physicians and psychiatrists. The increase was driven primarily by visits for anxiety and depression. The increase occurred in parents of different ages and across deprivation quintiles of their area of residence.
The rapid increase in use of mental health services by parents coincided with the onset of the pandemic and the imposition of NPIs that continued throughout the pandemic.2 This suggests an association between the COVID-19 pandemic and efforts to control it through NPIs and the rates at which parents sought care for mental health needs, particularly for anxiety and depression. This observed association is consistent with previous research on the role of women in parenting and related risks of anxiety and depression10–13 and with international studies conducted early in the COVID-19 pandemic on mental health in mothers of young children.12,14–19
There are a range of mechanisms through which the pandemic and associated NPIs could have impacts on mental health, including elevated stress and depression owing to concerns with potential illness from COVID-19, disruption in social supports, disruptions to work and finances, increased relational stress, worries about looking after children and their educational development, and a constant balancing of competing domestic and work demands.17,33
Limitations
This study used a quasi-experimental design to examine the association between the onset of the pandemic and NPI strategies used in Ontario and mental health visits by parents of children. This type of research cannot provide evidence of causality. Furthermore, given the wide range and variation in application of specific NPIs over time in Ontario,2 this study cannot provide evidence on the impact of specific NPIs. However, the short time between the imposition of NPIs and changes in mental health care utilization in these cohorts, and the sustained increase in use over 21 months, does suggest a fundamental change in mental health care utilization associated with the onset and aligned over time with the imposition of NPIs.
The fact that virtual care was a major component of this increased utilization of services does raise possible concerns that the increase in use of services was driven by this shift in modality of care. Research in Ontario showed a rapid increase in virtual outpatient care services at the outset of the pandemic for all conditions, including mental health services; however, for both overall and mental health services, the total number of visits (virtual and in person) decreased at the outset of the pandemic and was not back to prepandemic levels after 9 months.22 In our 2 cohorts, there was a shift to virtual care, as seen more generally, but it is important to note that virtual care delivery accounted for about 10% of care provided to our 2 cohorts in the prepandemic period (Appendix 1, Supplemental Table 1) and that the total number of visits (virtual and in person) increased beyond prepandemic rates quickly and remained elevated, unlike the overall trends.22 Furthermore, our results are consistent with a previous Ontario study21 that showed immediate, rapid and prolonged increases in immediate postpartum mental health service use. Nonetheless, some of the increase in rates might be the result of increased availability of virtual care and reduced barriers to previously unmet needs.
Our study linked parents to children at birth. We are not able to provide assurance that the birthing parent was still living with or parenting the child during the follow-up. We assume that most birthing parents remain connected in some way to that child. While it would have been ideal, we were unable to include nonbirthing parents in the study.
We used visits to physicians for mental health as the primary outcome. Mental health services provided by other professions or by physicians billing outside of OHIP are not included in this analysis. The OHIP physician billing data have been shown to be accurate in terms of billing claims for OHIP codes used in this study linked to the delivery of a mental health services for those diagnoses.31 However, these claims may not be sensitive in terms of capturing all potentially relevant mental health services provided by a physician to a member of one of our cohorts.31 This, combined with the lack of data on services from other providers or services provided by physicians outside of OHIP, means that this study does not provide evidence on all mental health service utilization by our cohorts in either the prepandemic or pandemic periods. The results are specific to OHIP billings for services in Ontario and may not be generalizable to other jurisdictions where containment policies, mental health service utilization data and population characteristics are different.
Conclusion
Over a 21-month pandemic period, we observed a rapid and sustained increase in physician visits for mental health diagnoses beyond what was expected for birthing parents of both younger and school-aged children. These increases were largely driven by services for mood, anxiety and depressive disorders. The increase occurred across provider types, age of parents and their deprivation quintile. The results of this large population-based study raise concerns about mental health impacts of the pandemic and the effort to contain it; if not adequately addressed, these could have long-term effects on parents and intergenerational impacts on their children.
Acknowledgements
The authors sincerely thank Minnie Ho and Alexandru Titeu for their support, helping to make this and other studies possible. Postdoctoral Fellowship support provided by the University of Toronto Institute for Pandemics, an academic centre dedicated to public health research and education on pandemic readiness, resilience and recovery, at the Dalla Lana School of Public Health.
Footnotes
Competing interests: Simone Vigod reports receiving royalties from UpToDate Inc. for authorship of materials related to depression and pregnancy. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Simone Vigod and Geoff Anderson contributed to the conception and design of the work. Join Moin, Lesley Plumptre, Natalie Troke, Irene Papanicolas, Walter Wodchis and Geoff Anderson contributed to the acquisition, analysis and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Sponsor — 303157 Canadian Institutes of Health Research grants, reference WI2-179943. Postdoctoral Fellowship funding provided by the University of Toronto Institute for Pandemics.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/6/E1093/suppl/DC1.
Data sharing: This study contracted ICES Data & Analytic Services (DAS) and used de-identified data from the ICES Data Repository, which is managed by ICES with support from its funders and partners: Canada’s Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research and the Government of Ontario. The data set from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: The opinions, results and conclusions reported are those of the authors. No endorsement by ICES or any of its funders or partners is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information and the Ontario Ministry of Health. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.