


Abstract
BACKGROUND: Indigenous people worldwide are disproportionately affected by diabetes and its complications. We aimed to assess the monitoring, treatment and control of blood glucose and lipids in First Nations people in Ontario.
METHODS: We conducted a longitudinal population-based study using administrative data for all people in Ontario with diabetes, stratified by First Nations status. We assessed age- and sex-specific rates of completion of recommended monitoring for low-density lipoprotein (LDL) and glycated hemoglobin (A1c) from 2001/02 to 2014/15. We used data from 2014/15 to conduct a cross-sectional analysis of rates of achievement of A1c and LDL targets and use of glucose-lowering medications.
RESULTS: The study included 22 240 First Nations people and 1 319 503 other people in Ontario with diabetes. Rates of monitoring according to guidelines were 20%–50% for A1c and 30%–70% for lipids and were lowest for younger First Nations men. The mean age- and sex-adjusted A1c level was higher among First Nations people than other people (7.59 [95% confidence interval (CI) 7.57 to 7.61] v. 7.03 [95% CI 7.02 to 7.03]). An A1c level of 8.5% or higher was observed in 24.7% (95% CI 23.6 to 25.0) of First Nations people, compared to 12.8% (95% CI 12.1 to 13.5) of other people in Ontario. An LDL level of 2.0 mmol/L or less was observed in 60.3% (95% CI 59.7 to 61.6) of First Nations people, compared to 52.0% (95% CI 51.1 to 52.9) of other people in Ontario. Among those aged 65 or older, a higher proportion of First Nations people than other Ontarians were using insulin (28.1% v. 15.1%), and fewer were taking no medications (28.3% v. 40.1%).
INTERPRETATION: As of 2014/15, monitoring and achievement of glycemic control in both First Nations people and other people in Ontario with diabetes remained suboptimal. Interventions to support First Nations patients to reach their treatment goals and reduce the risk of complications need further development and study.
Diabetes and its related complications are major contributors to morbidity and mortality worldwide.1–3 Indigenous populations in Canada and around the world are disproportionately affected by diabetes owing to the complex relations among colonization, social disadvantage, stress, trauma and metabolic health.4–7 In addition to our own work showing persistently higher rates of peripheral vascular disease, stroke, cardiac disease, renal dysfunction and ophthalmologic complications in Ontario First Nations,8–12 other Canadian and international studies also showed higher complication rates in diverse Indigenous populations.6,7,13–15
Glycemic control is fundamental to the management of diabetes and the prevention of complications.16 Glycated hemoglobin (A1c) is a reliable way to estimate the average level of glucose in the blood.17 Since A1c levels higher than 7.0% have been associated with an increased risk of microvascular complications,18–20 treatment guidelines suggest A1c should be measured every 3–6 months to ensure that glycemic goals are being met or maintained.21 Since people with diabetes also have an elevated risk for cardiovascular disease,22–24 management and control of cardiovascular risk factors, particularly lipids such as low-density lipoprotein (LDL) cholesterol, are also important.25–27 Guidelines further recommend that a full lipid profile be measured every 1–3 years, depending on cardiovascular risk, and suggest that LDL be consistently less than 2.0 mmol/L.28 Control of A1c and lipids has been shown to be associated with reduced morbidity and mortality in patients with diabetes.18,29–32
One possible reason for the high burden of complications among Indigenous people with diabetes may be failure to achieve control of these 2 key clinical parameters. We examined differences between Status First Nations people with diabetes in Ontario and all other Ontario residents with diabetes in rates of monitoring of A1c and lipids, achievement of targets for A1c and LDL outlined in clinical guidelines, and patterns of medication use to help attain these targets.
Methods
We conducted a retrospective population-based cohort study in Ontario, Canada. Data evaluated in this study were sourced from comprehensive linked health administrative data sets related to Ontario’s single-payer publicly funded health care system housed at ICES, an independent, not-for-profit organization. 33 The general approach including a description of the major data sets used and the characteristics of the study cohort are described in detail elsewhere.34 We created annual cohorts of the population with diabetes for each fiscal year between Apr. 1, 1995, and Mar. 31, 2015. All people from the Registered Persons Database (Ontario residents eligible for a health card) who were alive at the beginning of each year, had a prior diagnosis of diabetes (Ontario Diabetes Database),35 had contact with the health care system within the previous 7 years, and were aged 105 years or younger were included in these cohorts. In partnership with the Chiefs of Ontario, the project team conducted the reviews required under the ICES–Chiefs of Ontario Data Governance agreement to allow linkage to the Indian Register. The Indian Register lists all people who are registered with the federal government as members of a First Nation that is recognized under the Indian Act. This allowed us to identify people who were registered as having First Nations Status; all other Ontario residents were considered to be the population of “other people in Ontario.”
We measured rurality using the Rurality Index for Ontario, with the 3 categories of urban (0–9), semiurban (10–39) and rural (≥ 40), and “No score,” which represents primarily remote and small rural areas.36 We used the Rurality Index for Ontario rather than the 2017 Statistics Canada Remoteness Index as the latter was generated with the use of data that postdate our study and was not yet linked for use with the other data sets at ICES. We measured comorbidity using the Johns Hopkins’ Aggregated Diagnosis Groups (ADGs) (low = 4 or fewer, medium = 5–9, high = 10 or more).37 We used a combination of residence codes, recorded when people are admitted to an emergency department or hospital (information obtained from the Canadian Institute for Health Information Discharge Abstract Database and National Ambulatory Care Reporting System) and postal codes from the Registered Persons Database to determine which First Nations people were residing in First Nations communities.34
Statistical analysis
We calculated age- and sex-specific and adjusted rates of A1c and lipid monitoring for each fiscal year using data from the Ontario Health Insurance Plan and the definitions established by Health Quality Ontario (2 A1c measurements or 1 complete lipid profile in a year).38 We calculated age- and sex-standardized rates, along with γ-distributed 95% confidence intervals (CIs),39 using a direct standardization based on the 2001 Ontario census population.40 The numerator for the rate was those in the yearly cohort who received A1c or lipid monitoring (see Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.191039/-/DC1, for definitions). In addition, for the subset of people with a valid test result in the Ontario Laboratory Information System (OLIS), we assessed the proportion of people with diabetes whose A1c and lipid values were controlled.33 We categorized A1c levels as good (≤ 7%), fair (> 7.0 to < 8.5) or poor (≥ 8.5). A person was considered to have lipids under control if the LDL value was 2.0 mmol/L or less. For both A1c and lipid control analyses, the denominator was restricted to those with at least 1 test recorded in OLIS in 2014/15. For people with more than 1 result for a test, we selected the most recent value. We estimated age- and sex-adjusted proportions and differences using marginal estimates from logistic regression.41
We also assessed the use of glucose-lowering drugs among patients with diabetes who were 65 years or older at the beginning of 2014/15. To capture medication prescriptions for glucose-lowering drugs, we used the Drug Identification Number database to identify all glucose-lowering medications and linked these to the Ontario Drug Benefit Program database to capture prescription information. The Ontario Drug Benefit Program database includes only publicly funded medications, so this analysis was restricted to all people 65 years of age or older. We used drug records from Apr. 1, 2014, through Mar. 31, 2015, for this analysis. We assessed the pharmacotherapy regimen, the distribution of different classes of medication and types of insulin prescribed.
We conducted all analyses using SAS Enterprise Guide version 7.1 (SAS Institute).
Ethics approval
In addition to Ontario First Nations data governance processes, including review and approval by the Data Governance Committee, our project was reviewed and approved by the research ethics boards at Queen’s University and Laurentian University.
Results
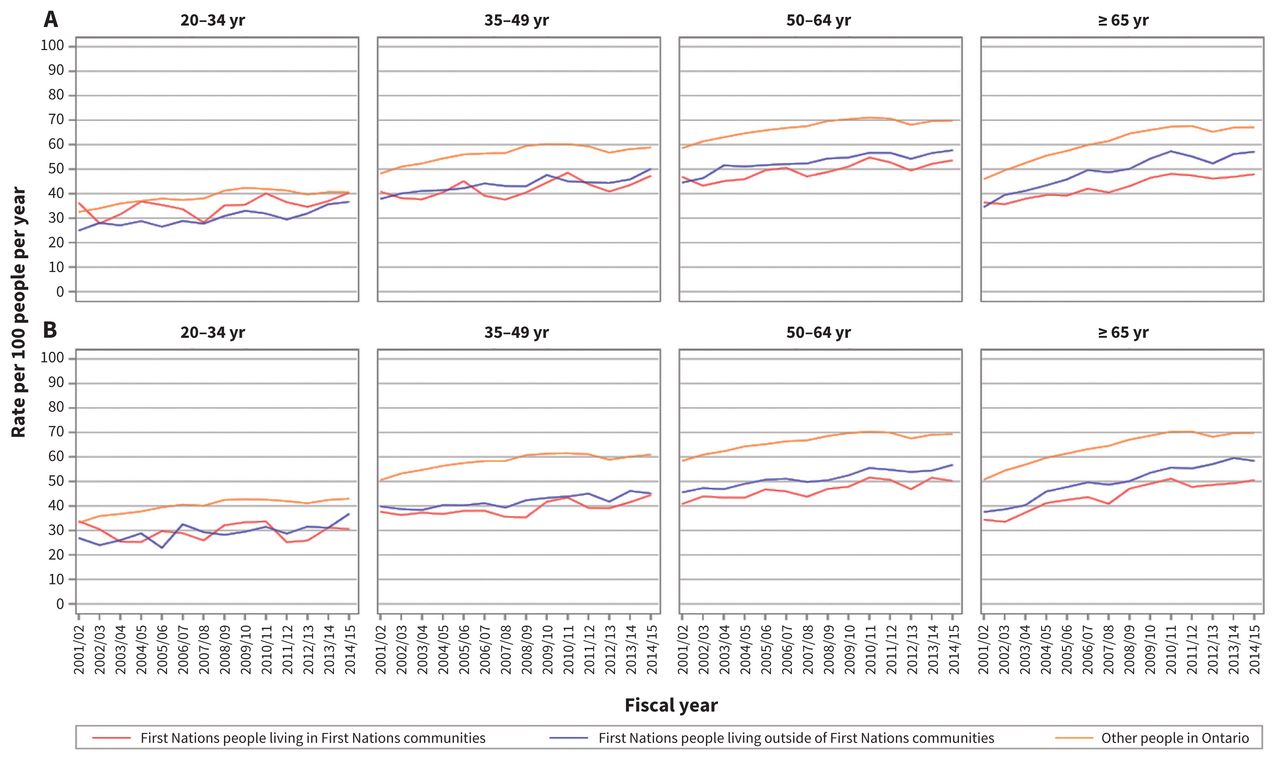
Table 1 presents the demographic characteristics of First Nations people living in or outside of First Nations communities and other people in Ontario with diabetes and the total population. The age- and sex-specific rates per 100 people with diabetes per year who were considered to have had completed A1c screening as recommended are presented in Figure 1. In 2014/15, these ranged from almost 20% among First Nations men aged 20–34 to just over 50% among other men in Ontario aged 65 or older. The age- and sex-specific rates of lipid screening per 100 people with diabetes per year are presented in Figure 2. In 2014/15, these ranged from 30% among First Nations men aged 20–34 living in First Nations communities to about 70% among other men in Ontario aged 50 or older, and other women in Ontario aged 50–64. Rates increased over time in all groups. They were significantly lower among First Nations people than other people in Ontario, with the lowest rates observed for younger people regardless of sex, First Nations status or location of residence. The gap between First Nations people and other people in Ontario was larger for men than for women and for older versus younger age groups, with absolute values ranging from 1%–2% for A1c monitoring in younger men to 20% for lipid monitoring in men and women aged 65 or older (Figure 2). For First Nations people aged 50 or older, lower rates were noted among those living in First Nations communities than those living outside First Nations communities.
Demographic characteristics of First Nations people living in or outside of First Nations communities and other people in Ontario with diabetes, 2014/15

Age- and sex-specific rates per 100 people per year of glycated hemoglobin monitoring completed as per guidelines (2 tests per year) among First Nations people with diabetes living in and outside of First Nations communities and other people with diabetes in Ontario, 2001/02 to 2014/15. (A) Women. (B) Men.

Age- and sex-specific rates per 100 people per year of lipid monitoring completed as per guidelines (once per year) among First Nations people with diabetes living in and outside of First Nations communities and other people with diabetes in Ontario, 2001/02 to 2014/15. (A) Women. (B) Men.
Among people with diabetes who had valid results for at least 1 A1c test in OLIS in 2014/15, the mean age- and sex-adjusted A1c level was higher for First Nations people than for other people in Ontario (difference 0.56%, 95% CI 0.54 to 0.59), a clinically significant finding (Table 2). Among people with diabetes who had valid results for at least 1 LDL test in OLIS in 2014/15, the mean age- and sex-adjusted LDL level was slightly lower for First Nations people than for other people in Ontario (difference −0.21 mmol/L, 95% CI −0.23 to −0.19) (Table 2), but this is likely not clinically significant. Good control of A1c was significantly less likely (47.9% [95% CI 46.6 to 48.0] v. 59.5% [95% CI 58.7 to 60.3]) and poor control significantly more likely (24.7% [95% CI 23.6 to 25.0] v. 12.8% [95% CI 12.1 to 13.5]) to be observed in First Nations people than in other people in Ontario. There were also differences between the groups in LDL levels, with First Nations people being more likely to be at target values (60.3% [95% CI 59.7 to 61.6] v. 52.0% [95% CI 51.1 to 52.9]). Among other people in Ontario, the proportion of those with good control of A1c increased with increasing degrees of comorbidity, whereas there was no consistent relation between comorbidity and A1c control in First Nations people. For both First Nations people and other people in Ontario, target levels for lipids were more likely to be achieved among those with higher levels of comorbidity.
Age- and sex-adjusted* glycemic and lipid control in First Nations people and other people in Ontario with diabetes,† 2014/15
Good glycemic control was related to rurality, with the highest level of control in urban areas and lowest in the most rural areas (Table 3). This was true for both First Nations people and other people in Ontario. There were no clinically significant differences in lipid control by rurality.
Good glycemic control and good lipid control by rurality among First Nations people and other people in Ontario with diabetes, 2014/15
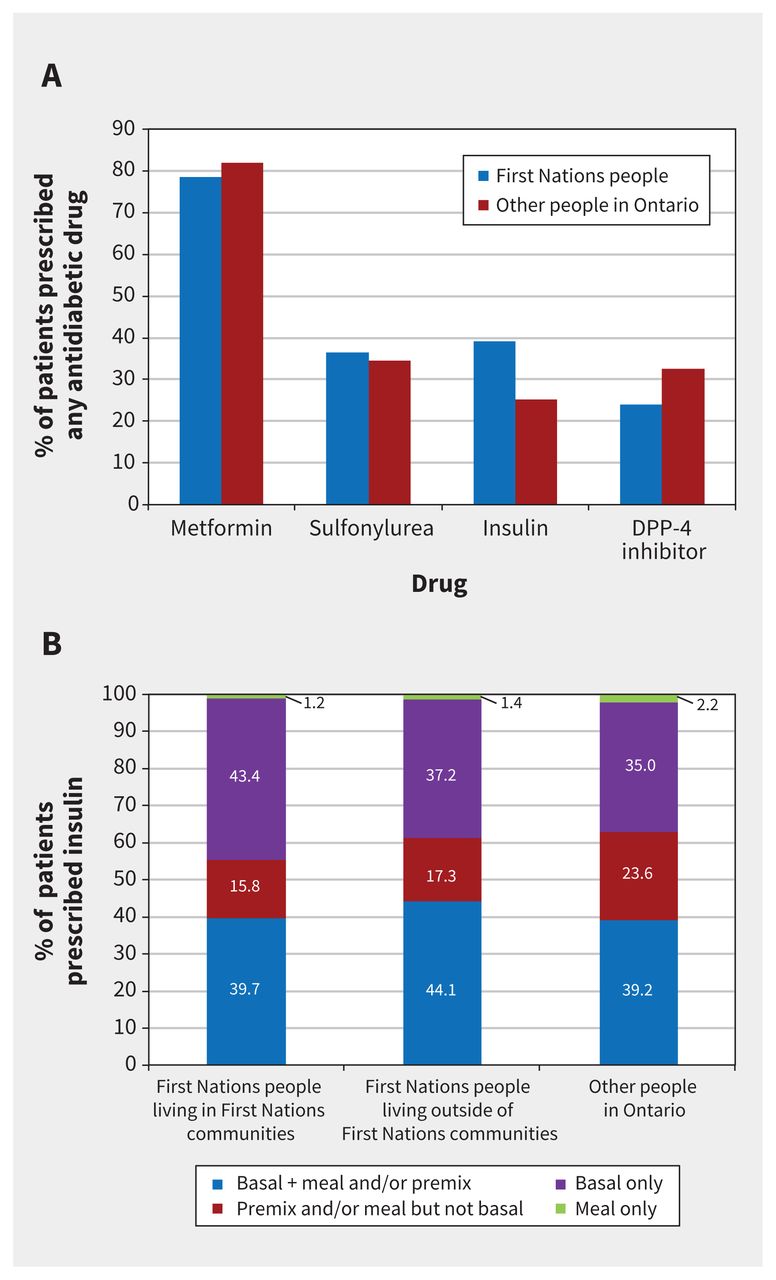
Figure 3 presents a summary of the types of pharmacotherapy regimens used by people with diabetes in 2014/15, and Figure 4 provides additional detail on the medication classes used. First Nations people were less likely to be taking no medications than other people in Ontario. They were more likely to be using insulin and less likely to have received a dipeptidyl peptidase 4 inhibitor than other people in Ontario. First Nations people were also more likely to be using basal insulin (alone or in combination) and less likely to be using premixed insulin or meal-only insulin than other people in Ontario.

Distribution of pharmacotherapy regimens among First Nations people and other people in Ontario aged 65 years or more with diabetes, 2014/15.

Medications for glycemic control by class among First Nations people and other people in Ontario aged 65 years or older with diabetes, 2014/15. (A) Oral agents and insulin. (B) Insulin by type. Note: DPP-4 = dipeptidyl peptidase 4.
We reported on the use of lipid-lowering agents, which is similar for First Nations people and other people in Ontario, in another paper.8
Interpretation
The frequency of testing to monitor glycemic control in Ontario increased between 2001/02 and 2014/15 but remained suboptimal, with 50% or less of all people with diabetes receiving 2 or more A1c tests per year; rates were as low as 20% among younger First Nations men. Rates of annual lipid testing were somewhat higher, but these tests were still completed in only about half of First Nations people and two-thirds of other people in Ontario with diabetes. In addition, among those with valid results, glycemic control was significantly worse among First Nations people than other people in Ontario with diabetes, with more than 30% of those in First Nations communities and 25% of those living outside First Nations communities having A1c levels of 8.5% or higher, compared to about 13% of other people in Ontario with diabetes. Conversely, lipid control was slightly better among First Nations people with diabetes. First Nations people were more likely than other people in Ontario to be using insulin and less likely not to be prescribed any glucose-lowering medications, but further analysis is required to determine the intensity and appropriateness of treatment, particularly as diabetes onset is more common at younger ages among First Nations people42 and the current analysis was limited to those aged 65 or older. The observed relations between increasing comorbidity and achievement of target A1c levels for other people in Ontario and of lipid targets for all groups may be due to higher levels of access to and use of health care services by these patients.43
Prior studies on treatment and control of diabetes in First Nations settings in Canada have also shown lower rates of monitoring and achievement of glycemic control. In the First Nations Diabetes Clinical Management Epidemiologic (CIRCLE) study,44 glycemic control, but not lipid control, was worse in First Nations patients with diabetes than in the general population in the earlier Diabetes in Canada Evaluation (DICE) cohort study, which used a similar methodology.45 The CIRCLE investigators also found high rates of treatment with glucose-lowering medications and low numbers of people receiving no medications among First Nations people.44 A study from Alberta showed that First Nations people with diabetes and without chronic kidney disease had lower rates of recommended A1c or LDL testing than their non–First-Nations counterparts and also were less likely to achieve A1c targets but not LDL targets.46
Improving glycemic control is an essential element of any strategy to limit the impact of diabetes on individuals and society. Because the OLIS data were acquired at ICES during the present study, we were unable to perform any longitudinal analysis of the links between the levels of glycemic control we observed and the high rates of complications reported in our other papers.8–12 However, it is highly likely that HbA1c level sare an important driver of the observed differences in outcomes, given the well-known strong association between glycemic control and complications of diabetes. Leiter and colleagues47 highlighted the difficulties in achieving glycemic control in their recent report combining results from the Diabetes Mellitus Assessment of Clinical Management in Ontario (DM-ACTION) and Diabetes Mellitus Improving Patient Care in Our Communities (DM-IMPACT) studies. Patient factors and therapeutic inertia on the part of clinicians were identified as key barriers to achieving targets.
Several studies have explored these issues as they relate specifically to First Nations people and communities in Canada. The authors of a mixed-methods study of 244 health care providers in 19 communities concluded that patient factors were critical but also expressed concern about the risk that this would lead to “patient blaming”; they noted that structural barriers such as the absence of local services or transportation difficulties were also important.48 Kulhawy-Wibe and colleagues49 conducted a qualitative study in 5 Alberta First Nations communities and concluded that there were many First-Nations–specific structural barriers to accessing diabetes self-management supports, including lack of local or culturally relevant resources. The Screening for Limb, I-Eye, Cardiovascular and Kidney (SLICK) complications program in Alberta developed mobile screening programs to help mitigate barriers to access,50 and the Transformation of Indigenous Primary Healthcare Delivery (FORGE AHEAD) program is evaluating quality-improvement interventions in multiple communities across Canada.51 Those investigators also reviewed the literature for best practices in diabetes and obesity prevention and treatment in Indigenous populations and noted that there is a pressing need for more studies of interventions to address this area.6,51
Research on patient and provider experiences in Canada has shown that there are important social and cultural drivers of diabetes outcomes among Indigenous adults that need to be addressed to help empower patients to achieve good control.52,53 The most recent Diabetes Canada guidelines recommend the use of care frameworks that are designed to help clinicians better understand the impacts of colonialism (including residential schools), ongoing inequities in care and structural barriers to care on their patients, and to develop strategies to create strong therapeutic relationships with patients, to help mitigate these challenges.7,54
Limitations
In addition to the general limitations related to using administrative data outlined by Slater and colleagues,34 there are some additional limitations particular to the present study. It is important to recognize that the diagnostic accuracy of the algorithm used to identify people with diabetes in First Nations populations is not known. In addition, this algorithm does not distinguish between type 1 and type 2 diabetes. The Ontario Laboratory Information System began incorporating hospital laboratory data on a regional basis, so hospital-based laboratories in northwestern Ontario, where there is a large First Nations population, were not contributing to OLIS during the period of the study. Our laboratory monitoring outcomes were based on Ontario Health Insurance Plan claims and are therefore missing data from hospital-based testing that is funded by global base budgets. In addition, there is no capture or reporting of results of point-of-care A1c tests, which may be conducted as part of organized diabetes care in some regions. It is difficult to be certain about the direction of bias these limitations may have introduced, but it is possible that they contributed to an underestimation of the differences in A1c control (owing to the relations between rurality and both A1c control and First Nations status) and an overestimation of the differences in up-to-date testing if hospital-based or point-of-care testing is more common for First Nations people than for other people. We also used only the most recent result for patients with more than 1 test result. We do not expect that this introduced systemic bias into the results comparing groups, as this was the case for all groups.
With respect to medication data, as we relied on the data for provincially funded drugs, any medications provided by private or federal funding programs such as the Non-Insured Health Benefits are not included, which may have contributed to underestimation of medication use. Since we limited our analysis of medications to people aged 65 or older, and since the provincial drug benefit system is the first-line insurer for all those in this age group in Ontario, including First Nations people, we feel that this is likely an issue only for medications that were not covered under the provincial health benefits plan (glucagon-like peptide-1 receptor agonists such as liraglutide and exenatide, and sodium–glucose transport protein 2 inhibitors such as dapagliflozin and canagliflozin were approved before March 2015 but were not on the Ontario Drug Benefit formulary). The Non-Insured Health Benefits program uses a formulary-based system similar to that of the Ontario Drug Benefit Program to determine eligibility for coverage of specific medications. There is a risk of misclassification for patient location, as address data from the Ontario Health Insurance Plan are not always current. We have mitigated this to the extent possible with administrative data by using the more current “residence code” for patients with hospital or emergency department encounters preferentially if there was a discrepancy. We were unable to account for socioeconomic status in our analyses. Finally, there may have been changes in outcomes since 2014/15, but these are likely to have been small in magnitude.
Conclusion
Monitoring for glycemic control remains inadequate for more than half of all Ontarians with diabetes and is even lower among First Nations people. The high rates of poor glycemic control noted for First Nations people are concerning, and glycemic control needs to be improved. This will require addressing many factors including difficulties accessing care, access to healthy foods and the long-term impacts of colonization. Robust studies of interventions designed to improve glycemic control by addressing these factors are urgently needed to inform changes in policy and practice.
Acknowledgements
The authors’ partner through the early design, implementation and final dissemination of this project was the Chiefs of Ontario. Their many member contributions were key to the content and quality of the project. Members of the project Patient Advisory Committee provided insightful and thoughtful input; their advice made a substantial contribution in shaping the work. The authors also acknowledge the First Nations people from Big Grassy River First Nation, Alderville First Nation, Caldwell First Nation, Six Nations of the Grand River and Moose Cree First Nation with diabetes who shared their personal experiences. The authors also thank Robyn Rowe for her contributions in reviewing key background literature and supporting the engagement of the study team with community partners, and Sue Schultz and Rahim Moineddin for their contributions to data set creation and cleaning, and to statistical analysis.
Footnotes
Competing interests: Michael Green has received consulting fees from Health Canada’s First Nations and Inuit Health Branch and grants for related research from the Canadian Institutes of Health Research and the Ontario Ministry of Health and Long-Term Care. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Michael Green, Baiju Shah, Carmen Jones and Jennifer Walker conceived of and designed the study, analyzed the data and drafted the manuscript. Morgan Slater and Shahriar Khan contributed to data analysis and drafting of the manuscript. All of the authors interpreted the data, revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by an IMPACT award from the Ontario SPOR SUPPORT Unit, which is supported by the Canadian Institutes of Health Research and the Province of Ontario. Additional support was provided to Michael Green through the Brian Hennen Chair in Family Medicine, and to Jennifer Walker through a Tier 2 Canada Research Chair in Indigenous Health and by ICES. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care.
Data sharing: The data set from this study is held securely in coded form at ICES. Although data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access. The full data set creation plan and underlying analytic code are available from the authors on request, with the understanding that the programs may rely on coding templates or macros that are unique to ICES.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information and the MOHLTC. The analyses, conclusions, opinions and statements expressed in this paper are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
- Accepted May 5, 2020.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Population-based birth cohort study on diabetes in pregnancy and infant hospitalisations in Cree, other First Nations and non-Indigenous communities in Quebec
- Diabetes during pregnancy among Metis people in Alberta: a retrospective cohort study
- Health care costs associated with hepatitis C virus infection in First Nations populations in Ontario: a retrospective matched cohort study
More in this TOC Section
Similar Articles

