


Abstract
Background: It is unclear whether there are sex-based differences in use of palliative care near the end of life. The objective of this study was to measure the association between sex and palliative care use.
Methods: We performed a population-based retrospective cohort study of all patients aged 18 years or older in the last year of life who died in Ontario, Canada, between 2010 and 2018. The primary exposure was patient biologic sex (male or female). The primary outcome was receipt of physician-delivered palliative care; secondary outcomes were approach to in-hospital palliative care and sex concordance of the patient and referring physician. We used multivariable modified Poisson regression to measure the association between patient sex and palliative care receipt, as well as patient–physician sex concordance.
Results: There were 706 722 patients (354 657 females [50.2%], median age 80 yr [interquartile range 69–87 yr]) in the study cohort, 377 498 (53.4%) of whom received physician-delivered palliative care. After adjustment for age and selected comorbidities, female sex was associated with a 9% relative increase (adjusted relative risk [RR] 1.09, 95% CI 1.08–1.10) in receipt of physician-delivered palliative care. Female patients were 16% more likely than male patients (adjusted RR 1.14, 95% CI 1.14–1.18) to have had their first hospital admission in their final year of life categorized as having a likely palliative intent. Female patients were 18% more likely than male patients (RR 1.18, 95% CI 1.17–1.19) to have had a female referring physician, and male patients were 20% more likely than female patients (adjusted RR 1.20, CI 1.19–1.21) to have had a male referring physician.
Interpretation: After adjustment for age and comorbidities, male patients were slightly less likely than female patients to have received physician-delivered palliative care, and female patients were more likely than male patients to have had their first hospital admission in their final year of life categorized as having a likely palliative care intent. These results may reflect a between-sex difference in overall end-of-life care preferences or sex differences in decision-making influenced by patient-specific factors; further studies exploring how these factors affect end-of-life decision-making are required.
Disparities in access to health care have led to increasing calls for research to identify and address inequities in health care delivery.1 Prior research has identified sex-based disparities in both the intensity and the frequency of health care services, including hospital admission, access to home-based end-of-life care and use of life-sustaining interventions at the very end of life, accessed by male and female patients.2–5
Palliative care improves quality of life, reduces symptom burden, and is associated with a reduction in use of health care services, an increase in quality-adjusted survival and an overall substantial cost-savings among patients with terminal life-limiting conditions.6–12 There remains considerable uncertainty about potential disparities in physician-delivered palliative care between male and female patients at the end of life. Prior research suggests that, in the province of Ontario, Canada, adult males were less likely than adult females to receive palliative care at the end of life.13–17 However, these findings were part of secondary analyses intended to be hypothesis-generating. Therefore, the objective of the present study was to measure the association of patient sex with physician-delivered palliative care in the last year of life. We also explored several patient- and provider-level factors that may potentially drive sex-based differences in palliative care use.
Methods
Data sources
We conducted a population-based retrospective cohort study in Ontario, Canada, using linked clinical and health administrative databases (Appendix 1, Supplementary Tables S1 and S2, available at www.cmajopen.ca/content/11/6/E1025/suppl/DC1). The administrative data sets used in this study were linked by means of encoded identifiers at the patient level and analyzed at ICES. Ontario is Canada’s most populous province, with more than 15 million people. All residents of Ontario have access to necessary institutional care (e.g., hospital, rehabilitation), outpatient care and physicians’ services. Administrative data generated during care delivery for all Ontarians are routinely collected, captured and stored at ICES. Details of the linked administrative databases used in this study, as well as the information captured from each database relevant to the study, can be found in Appendix 1, Supplementary Table S2.
Study design and setting
We included all adults (age ≥ 18 yr) in Ontario who died between January 2010 and December 2018. We chose this period as there were reliably complete and updated data in the linked health administrative databases used in the study for our decedent cohort. People were excluded if 1) they were classified in the sudden-death illness trajectory according to the cause of death on their death certificate (Appendix 1, Supplementary Table S3); 2) they did not have a valid Ontario health card number within the 365 days before their death, or were not eligible for Ontario health care benefits within the 5 years before death and were therefore ineligible to receive health care services; 3) they were not Ontario residents at the time of death; 4) data on sex or date of death were missing; and 5) they were not a new user of palliative care (prevalent user), that is, they had received 2 or more palliative care visits in the year before the last year of life (720–360 d before death) that were less than 180 days apart. The last criterion reflects a new-user design whose purpose is to reduce the confounding and bias that typically accompany inclusion of data from prevalent users in observational studies such as this one.18 The use of this design led to the exclusion of prevalent users of palliative care, who may inherently have had different survivorship and different cumulative responses to sustain palliative care intervention than other decedents.
Beyond sex, this study captured age, income quintile, rurality, recent immigrant status, comorbidities, frailty and cause of death. We stratified male and female patients into 4 end-of-life illness trajectories on the basis of their cause of death: cancer (terminal illness), organ failure, dementia (frailty) and sudden death. Decedents categorized in the last trajectory were excluded from the analysis. These trajectories, which cover a wide range of causes of death/disease codes, have been shown to strongly predict palliative care receipt at the end of life, with those in the terminal illness group having the highest probability of receiving palliative care.13 The definitions and uses of these trajectories have been extensively described and validated elsewhere.13,19–22 Further details of International Statistical Classification of Diseases and Related Health Problems, 10th Revision, codes used are given in Appendix 1, Supplementary Table S3.
Specific provider demographic characteristics captured included sex, location of training, location of practice and specialty of practice. These provider-level factors have been shown to influence end-of-life care delivered by physicians.23
We defined patient sex as male or female and identified it using the Registered Persons Database, which contains detailed demographic information for all Ontarians eligible to receive insured health care services in the province. As of 2017, Ontario made amendments to its legislation, allowing for recognition of people who are transgender, nonbinary or two-spirit with the designation of a third category aside from the traditional male and female categories. Before this, all decedents in the province were categorized based on binary biologic sex (male or female). Given the recency of this change, as well as the timeline of this study, these changes were not reflected in the provincial health administrative data used. As a result, we used biologic sex rather than gender as the primary exposure.
This study is reported in accordance with guidelines for The Reporting of Studies Conducted Using Observational Routinely Collected Health Data (RECORD).24
Outcome
The primary outcome was receipt of any physician-delivered palliative care in any setting. Physician-delivered palliative care was identified using a specific set of palliative care physician fee codes that have been widely used in prior palliative care research. This method identifies physician-delivered palliative care with a sensitivity of 76% and specificity of 97.8% (Appendix 1, Supplementary Table S4).2,10,13,15–17,25–32 Furthermore, physician-delivered palliative care identified in this manner is associated with important end-of-life outcomes such as likelihood of dying at home and receipt of palliative home care.25,29,31,33 We also reported relative sex proportions of prevalent users.
Our study had 2 secondary outcomes. The first was approach to care, including the potential involvement of palliative care during the first hospital stay in the last year of life. We assessed this using a previously described and validated method that categorizes hospital stays as palliative intent likely, palliative intent unlikely or no palliative intent (Appendix 1, Supplementary Table S5).34–37 Briefly, this categorization reflects the preferences of and care received by the patient, including status of their most responsible provider as a palliative practitioner and in-hospital palliative care consultations. Previous studies by our group have shown that varying levels of palliative care intent can predict important end-of-life outcomes, including receipt of community/home palliative care and acute care hospital admissions, as well as overall cost of end-of life-care.34,36,37 The components of this categorization (which include most responsible diagnosis and most responsible provider) are captured at the patient level by trained chart abstracters at the Canadian Institute for Health Information using methodology that has been validated by the institute elsewhere. 38 Subsequently, we applied a previously described algorithm (Appendix 1, Supplemental Table S5B) that used these components to stratify each hospital admission into 1 of the 3 end-of-life illness trajectories (cancer, organ failure or dementia).
Second, we also measured the sex concordance between decedent patients who received palliative care and the physicians who referred them for palliative care.
Statistical analysis
We used multivariable modified Poisson regression, which estimates adjusted relative risk (RR) with robust standard errors, to measure the association between patient sex and receipt of palliative care, and the association between patient sex and concordance of patient–physician sex in referral to palliative care.39 We performed all patient-level analyses in subgroups defined by illness trajectory. We used multivariable multinomial regression to measure the association between patient sex and approach to care during the first hospital stay in the last year of life. For patients who received palliative care in the last year of life, we used a modified Poisson regression to measure the association between patient sex and the sex of the first provider who referred the patient for palliative care in order to identify patient–provider sex concordance. All consultations rendered by a physician in Ontario require the referring physician to be included as part of the claim. We determined the sex of the referring physician using the ICES Physician Database. As part of this analysis, referring physician sex was the main exposure, and patient sex was the outcome. The analysis focused on the association between male referring physician and male patient, and female referring physician and female patient. We adjusted patient models for age (by age group) and the presence of chronic conditions, including cancer, chronic kidney disease, cirrhosis, coronary artery disease, dementia, diabetes, hypertension and nonpsychotic mental health conditions (e.g., depression, anxiety), based on inclusion in ICES disease prevalence cohorts. We used standardized differences to describe the difference in baseline characteristics between male and female patients. Variables were selected for inclusion in the analytical models based on the expertise of our clinical research team and recent literature on important factors related to sex-based differences in care, as well as variables for which there was a standardized difference greater than 0.1 between male and female patients.40
We adjusted physician-related models for physician age, specialty, location of practice and location of training.
We performed all analyses using SAS version 9.4 (SAS Institute).
Ethics approval
The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board.
Results
Between January 2010 and December 2018, 857 970 people died in Ontario, of whom 151 248 were excluded for the following reasons: age 18 years or younger (n = 4398), not eligible for provincial health care benefits during the last year of life (n = 5060) or in the 5 years before the eligibility date (n = 12 768), received 2 or more palliative care visits in the year before the last year of life/eligibility date that were 180 days or less apart (n = 39 281), cause of death categorized as sudden death (n = 28 524), cause of death not captured in other categories (n = 46 238) and no known cause of death (n = 9897). The remaining 706 722 patients (354 657 females [50.2%], 352 065 males [49.8%]) were included in the study cohort. Information with regard to biologic sex and date of death was complete for all patients. The patients’ demographic characteristics are presented in Table 1. A total of 264 709 patients (37.5%) were categorized as having organ failure as the cause of death (organ failure trajectory), 225 608 (31.9%) as having dementia (frailty trajectory) and 216 405 (30.6%) as having cancer (terminal illness trajectory). Male and female patients were equally represented in all 3 illness trajectories.
Patient characteristics
Palliative care use
Overall, 377 498 patients (53.4%) received palliative care in the last year of life, 192 022 female patients (54.1%) and 185 476 male patients (52.7%) (Table 1). After we controlled for age and selected comorbidities, female patients were 9% more likely than male patients to have received physician-delivered palliative care (adjusted RR 1.09, 95% CI 1.08–1.10, absolute difference 1.4%, n = 9894) (Table 2; Appendix 1, Supplementary Figure S1). There was a gradient of sex differences in palliative care delivery on the basis of cause of death, with the largest difference seen among adults who died from organ failure, followed by dementia and cancer. Concordantly, a higher proportion of prevalent users of palliative care were female than male (Appendix 1, Supplementary Table S9).
Probability of receiving physician-delivered palliative care in the last year of life according to patient sex, by cause of death*
Multivariable analysis of approach to palliative care
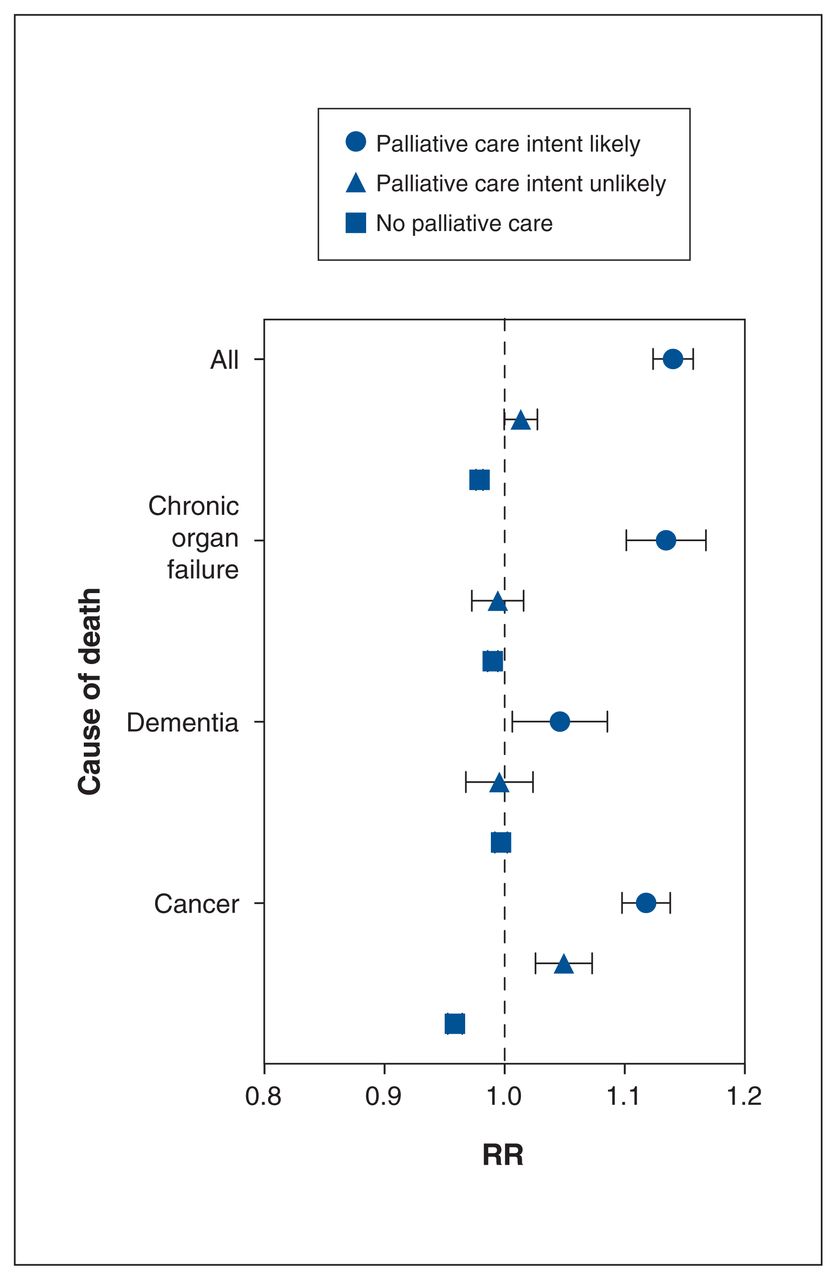
After we controlled for age and comorbidities, female patients were 16% more likely than male patients to have had their first hospital admission in their final year of life categorized as having a likely palliative care intent (adjusted RR 1.14, 95% CI 1.14–1.18, absolute difference 4.8%, n = 3388) (Figure 1; Appendix 1, Supplementary Table S6). Male and female patients were equally likely to have had their hospital admission categorized as having an unlikely palliative care intent. Female patients were 5% less likely than male patients to have had their hospital admission categorized as having no palliative care intent (adjusted RR 0.95, 95% CI 0.95–0.96, absolute difference 4.8%, n = 18 007).
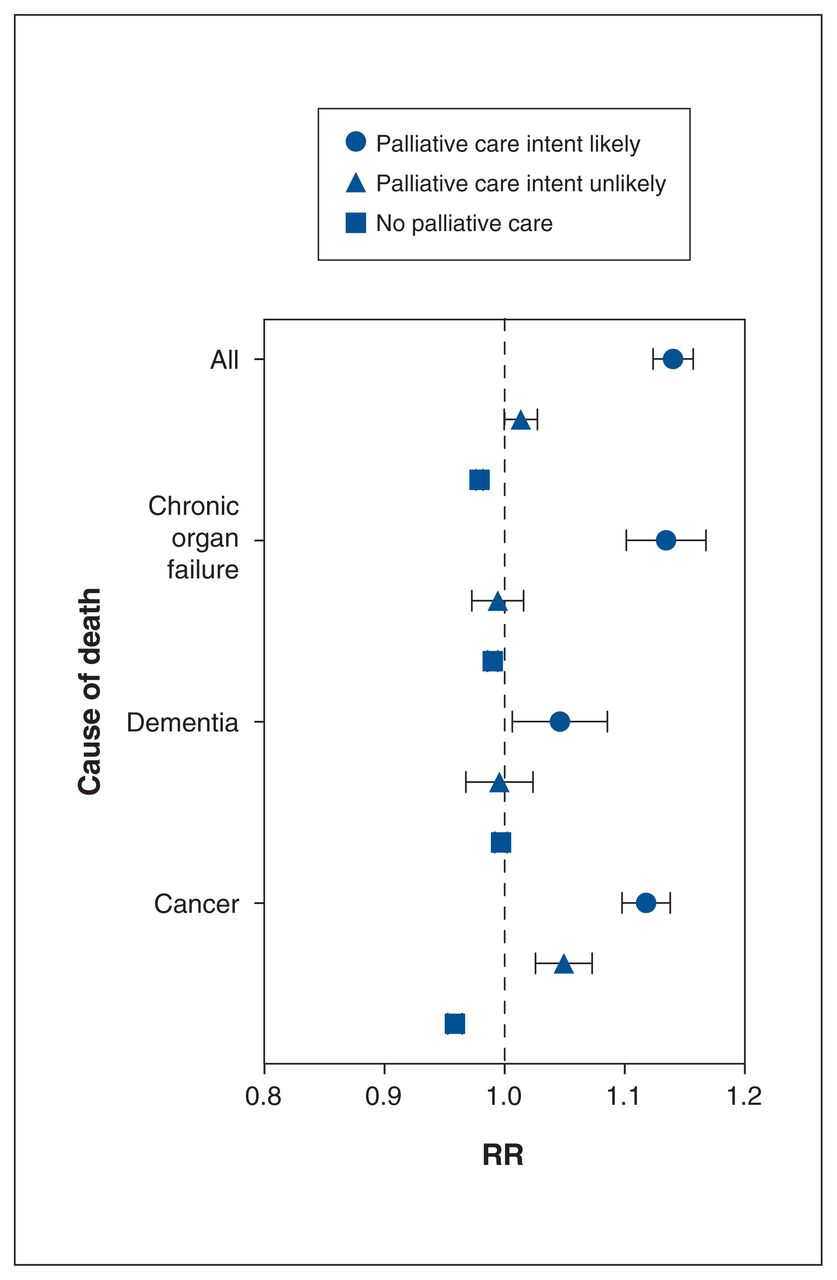
Probability of a palliative approach to care during the first hospital admission in the last year of life, female versus male sex, among 706 722 adults who died between January 2010 and December 2018 in Ontario, Canada, by cause of death. Models were adjusted for age and chronic conditions. Note: RR = relative risk. Error bars represent 95% confidence intervals.
Multivariable analysis of physician sex for patients referred for palliative care
Female physicians were 18% more likely to have referred female patients than male patients for palliative care (adjusted RR 1.18, 95% CI 1.17–1.19, absolute difference 13.9%, n = 29 458). The magnitude of this finding was most pronounced among adults who died from cancer, followed by organ failure and dementia (Figure 2A; Appendix 1, Supplementary Table S7). Male physicians were 20% more likely to have referred male patients than female patients for palliative care (adjusted RR 1.20, CI 1.19–1.21, absolute difference 3.0%, n = 16 270) (Figure 2B; Appendix 1, Supplementary Table S8).
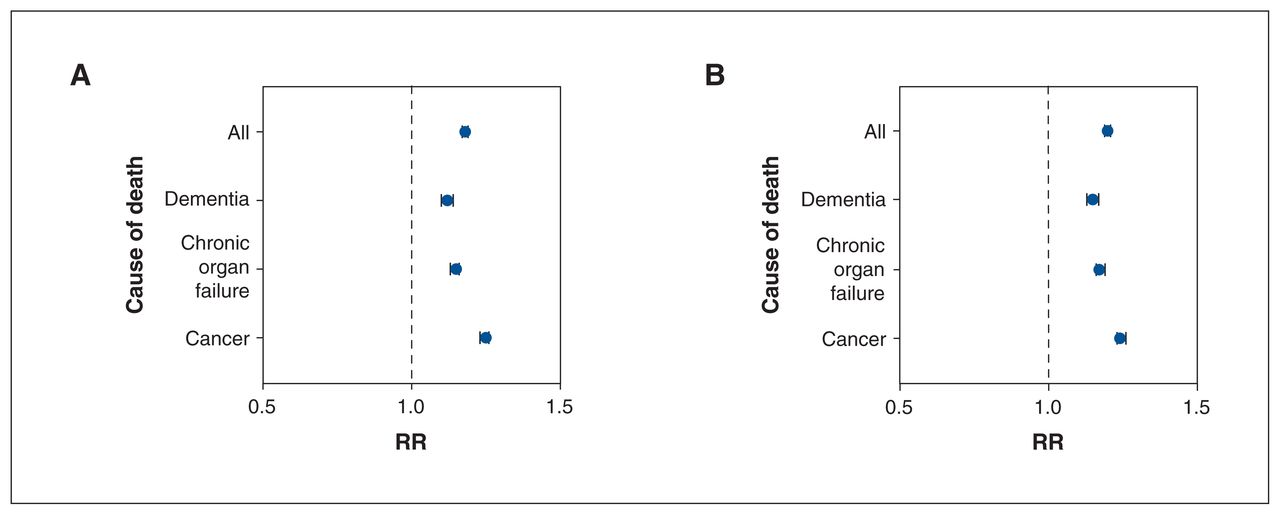
Probability that a female patient versus a male patient would be referred to palliative care by a female physician (A) and that a male patient versus a female patient would be referred by a male physician (B). Models were adjusted for patient age, chronic conditions, physician sex, location of practice and location of medical training, and were stratified by cause of death. Note: RR = relative risk. Error bars represent 95% confidence intervals.
Interpretation
This population-level cohort study of 706 722 adults in the last year of life whose cause of death was categorized as cancer (terminal illness), organ failure or dementia (frailty) showed that a higher proportion of female patients than male patients received physician-delivered palliative care in the last year of life. After adjustment for age and comorbidities, female sex was associated with a relative increase of 9% in palliative care use. This finding was consistently observed among patients with varying causes of death but most prominently among those who died from organ failure or dementia. The proportions of patients with organ failure, dementia and cancer as the cause of death were consistent with previous estimates for the Ontario population.13 Interestingly, a higher proportion of prevalent palliative care users were also found to be female.
Regarding our primary finding, female patients’ hospital admissions may have triggered out-of-hospital palliative care referrals, resulting in initiation of end-of-life palliative services. 35 Interestingly, the associated effect of sex concordance between patients and their referring provider was equal among male and female patients, with male physicians being more likely to have referred male patients for palliative care, and female physicians being more likely to have referred female patients. It is therefore unlikely that provider and patient sex concordance accounts for our primary finding. This is in contrast to prior studies showing that patient–provider sex concordance significantly affected health outcomes in areas such as cancer screening and management of cardiovascular disease.41–43 Our finding that sex differences in palliative care receipt were larger among patients who died from organ failure or dementia than among those who died from cancer. This may reflect institutional efforts to integrate palliative care into routine cancer care, such that patients with cancer may have had more opportunities to receive palliative care, which would mitigate the associated effects of patient sex on use.17,25
Our main finding is in keeping with prior exploratory studies that suggested that a sex difference in physician-delivered palliative care may exist.14–16,25 This sex difference may have important downstream implications for other end-of-life outcomes that are affected by palliative care receipt, such as location of death, receipt of palliative home care and acute hospital admission.6–12 Our study not only builds on this work but also explored patient- and provider-level factors that may explain this sex difference. What still remains unclear is whether the sex difference in palliative care receipt that we observed represents a fundamental difference in end-of-life care preferences between male and female patients, or sex-specific decision-making influenced by factors such as caregiver preferences, marital and financial status, race and socially constructed gender roles. Previous studies have identified sex-based differences in end-of-life decision-making.44–47 Although these were small regional studies, they showed that, in contrast to female patients, male patients and their caregivers had a consistent preference to pursue end-of-life care with a curative intent.
There have been renewed calls to identify and address health inequities in the health care system as a result of the disparities highlighted during the COVID-19 pandemic.48 To develop policies aimed at minimizing potential inequities in health care, a better understanding of sex- and gender-specific end-of-life decision-making and use of palliative care is required. This will require small-scale studies in which gender and other patient-specific variables can be captured in a more detailed fashion. There is a paucity of patient-level data exploring how patient-specific factors such as income and caregiver availability may influence the decisions that patients make at the end of their life. To gain a better understanding of this issue, patient-level survey data will likely be required.
Limitations
Given this study’s retrospective observational nature, our results reflect associations and are not causal. Although we systematically adjusted for a comprehensive list of important confounding variables that differed between male and female patients, the possibility of residual confounding remains. There are many important variables that may influence a patient’s probability of receiving palliative care that are not routinely collected as part of health administrative data in Ontario; for example, these databases capture limited information with regard to gender as a social construct, marital status, education level and ethnicity. Beyond this, other important variables such as caregiver, financial and functional status are not captured. We attempted to mitigate this by measuring a comprehensive set of gender-related variables including socioeconomic status, rurality and immigrant status. Similarly, sex differences in disease prevalence not accounted for in this study may have influenced the between-sex differences in use of palliative care across all causes of death. However, these sex-based differences were persistent in all analyses among different subgroups of cause of death, including cancer, in which there were more males than females. Furthermore, we did not adjust for physician factors in our primary analysis. We did, however, adjust for physician-level factors in our secondary analysis of the first provider who referred the patient for palliative care, where these factors are more likely to be influential.
Our sex concordance analysis may help elucidate a potential mechanism to explain our main findings. However, our sex concordance findings may simply reflect the fact that patients who receive palliative care are more likely to obtain medical care from someone of their own sex rather than the opposite sex.
This study did not capture palliative care delivered by other health care providers such as nurse practitioners, spiritual care providers and social workers. Any potential sex-based differences in the palliative or end-of-life care delivered by these providers, including care that may be provided in nonphysician palliative care models, remain unknown. Furthermore, it is possible that this study did not identify palliative care delivered by physicians under alternative fee codes or funding models not included in our analysis, such as unbilled palliative care that may be delivered by a family physician to a patient rostered in their practice. It is unclear what effect, if any, the noninclusion of this care may have had on our results. However, the method we used to identify physician-delivered palliative care is robust and has been widely used.2,10,13,15–17,25–32
We used a previously described methodology to categorize approach to in-hospital palliative care that relies on abstraction of the important aspects of the hospital admission, such as most responsible diagnosis and most responsible provider.34–37 There is a possible risk of misclassification with this method; however, the Canadian Institute for Health Information has developed validated mechanisms for maintaining data quality and reliability within the Discharge Abstract Database, which minimizes the risk of misclassification.38
Palliative care initiated and provided in different care settings such as in hospital, at home or in the ambulatory clinic may involve a different distribution of physicians. It is possible that patient assignment to a specific physician may have differed according to the location in which their care was provided, and this may have introduced unmeasured confounding. Given that many patients in this study received palliative care in multiple locations from the same or different physicians, it was not feasible to control for location of palliative care receipt in the primary analysis.
Finally, our study reflects patterns of palliative care practice that may not apply to other jurisdictions, especially those without a single-payer health care insurance system. For example, in other regions internationally, there may not be the same ready access to institutional palliative care or physicians practising as palliative care specialists as in Ontario.
Conclusion
In this population-level cohort study of Ontario adults in the last year of life whose death was due to cancer, organ failure or dementia, male patients were slightly less likely than female patients to have received physician-delivered palliative care. Female patients were more likely than male patients to have had hospital admissions at the end of life categorized as having a likely palliative care intent. These results may reflect a between-sex difference in overall end-of-life care preferences or sex differences in decision-making influenced by patient-specific factors. Further studies exploring how these factors affect end-of-life decision-making are required.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Disclaimer: Nathan Stall is an associate editor with CMAJ and was not involved in the editorial decision-making process for this article.
Contributors: Kevin Gitau, Kieran Quinn and Chaim Bell conceived and designed the study. Anjie Huang acquired the data, Anjie Huang, Kieran Quinn and Kevin Gitau analyzed the data, and Kevin Gitau and Kieran Quinn interpreted the data. Kevin Gitau drafted the manuscript. Kieran Quinn, Chaim Bell, Sarina Isenberg, Nathan Stall and Jonathan Ailon supervised the study. All authors revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The data set from this study is held securely in coded form at ICES. Although data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors on request, with the understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/6/E1025/suppl/DC1.
Funding: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. This study received specific funding from the Physicians Services Incorporated Foundation (grant R21-08).
Disclaimer: The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario Ministry or Health or the Ministry of Long-Term Care is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors and not necessarily those of CIHI.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.